Contents and gallery
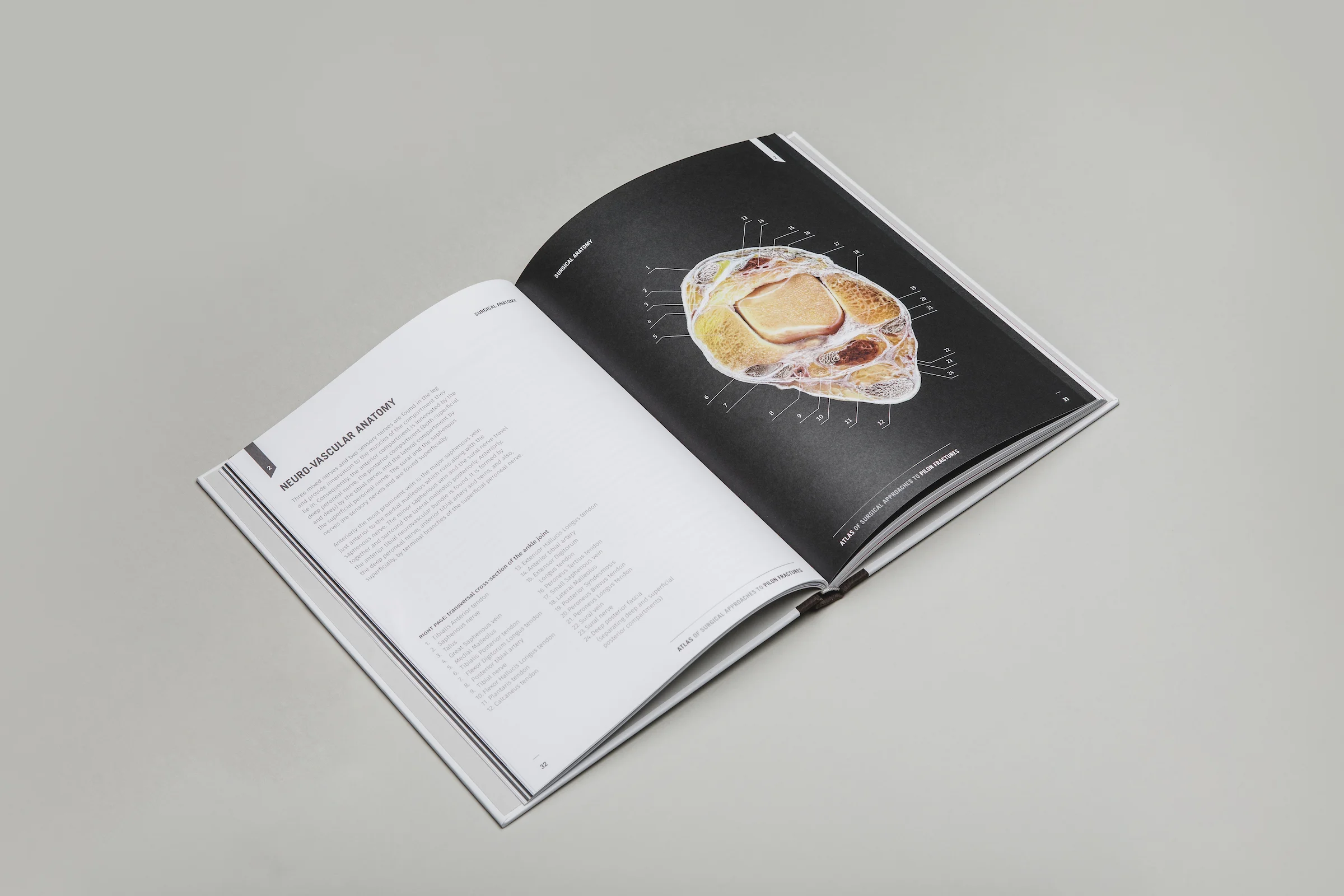
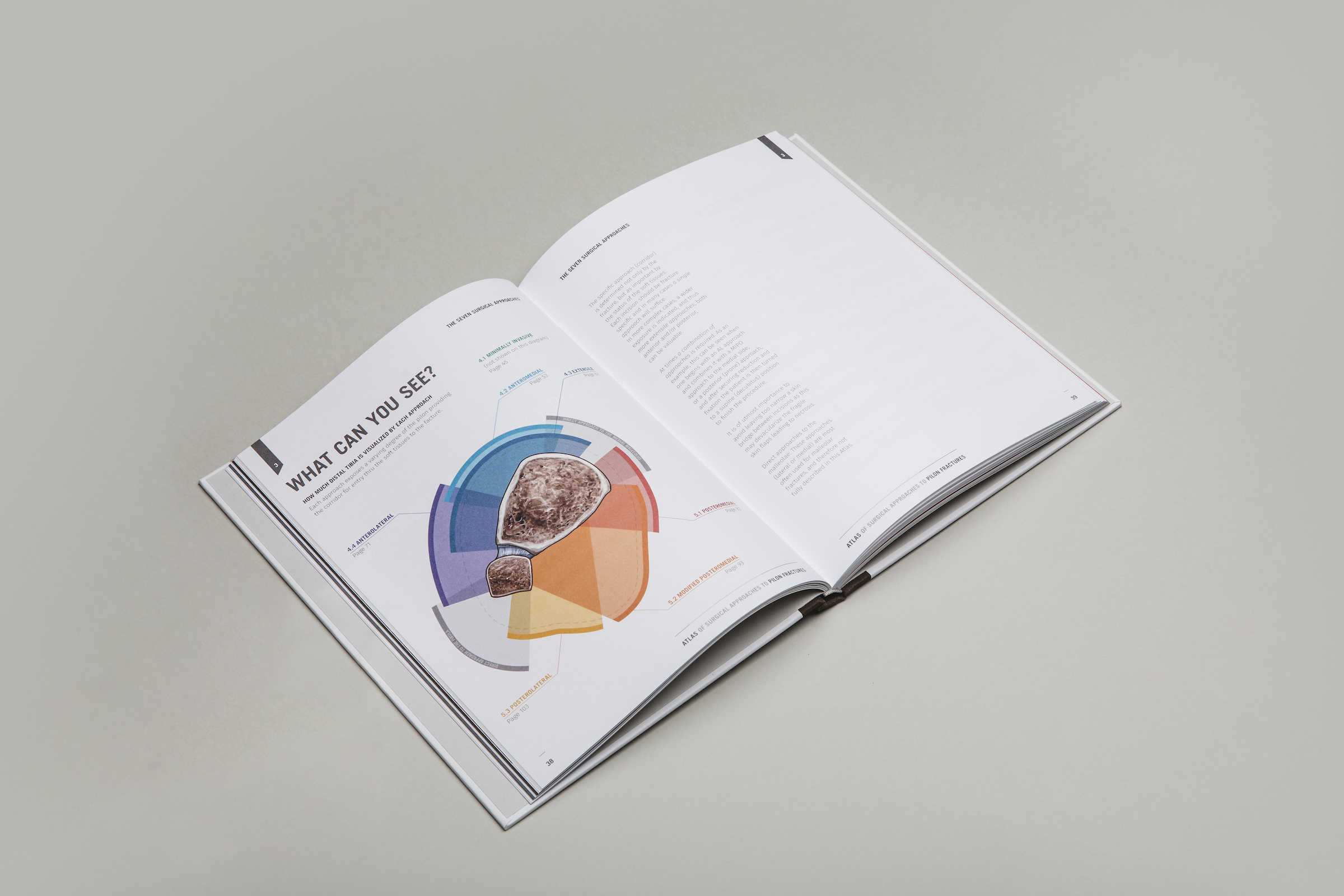



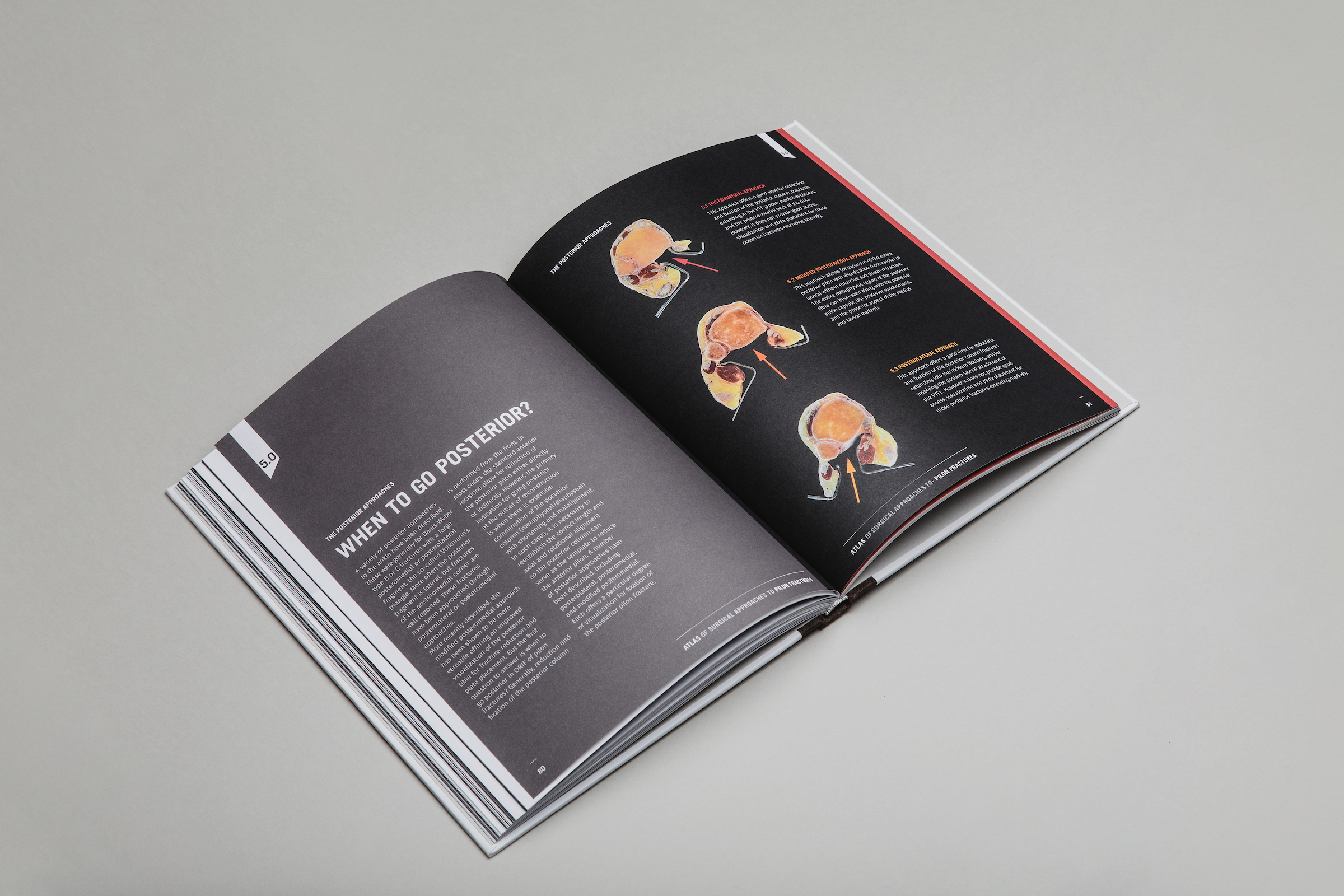
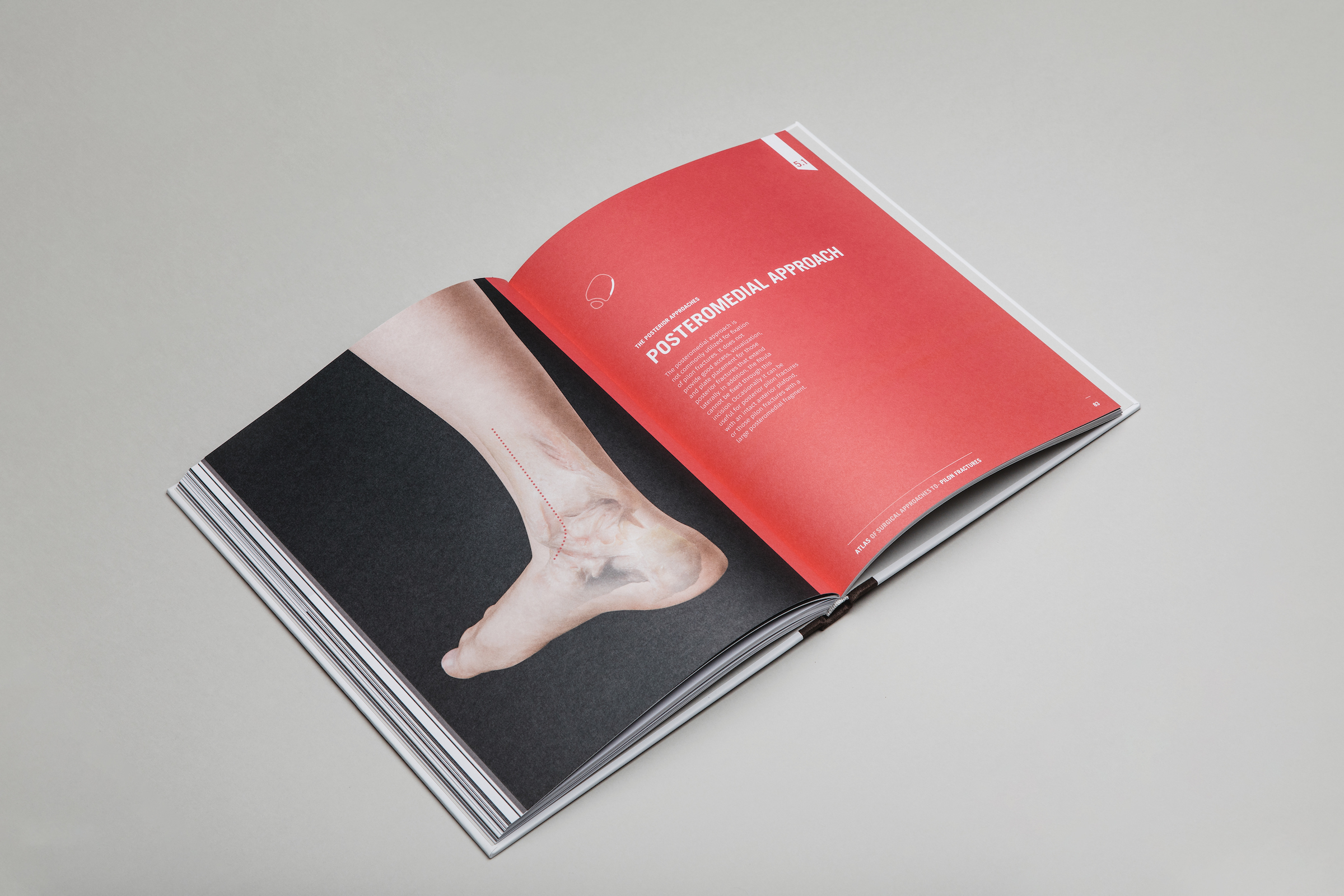
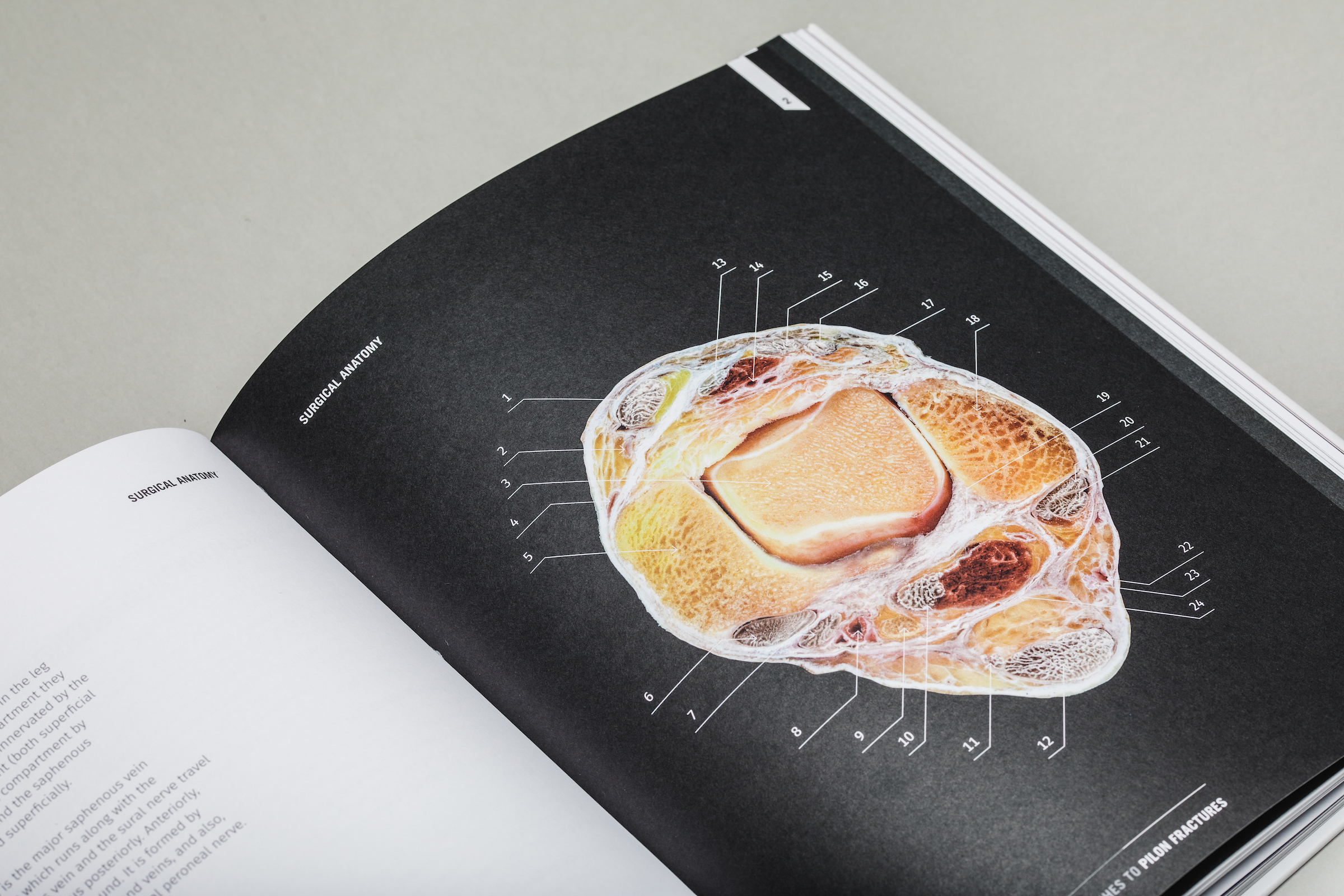

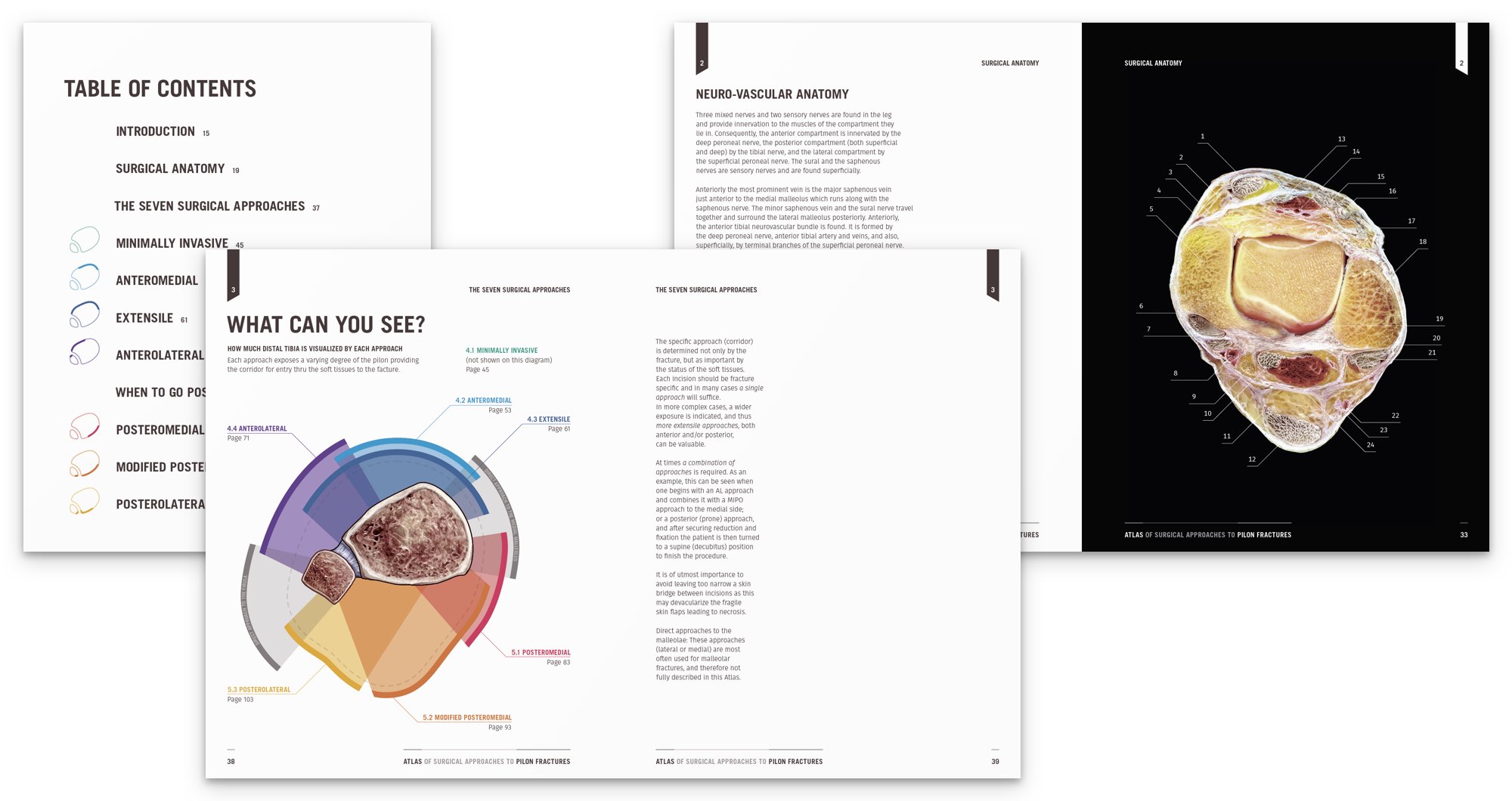
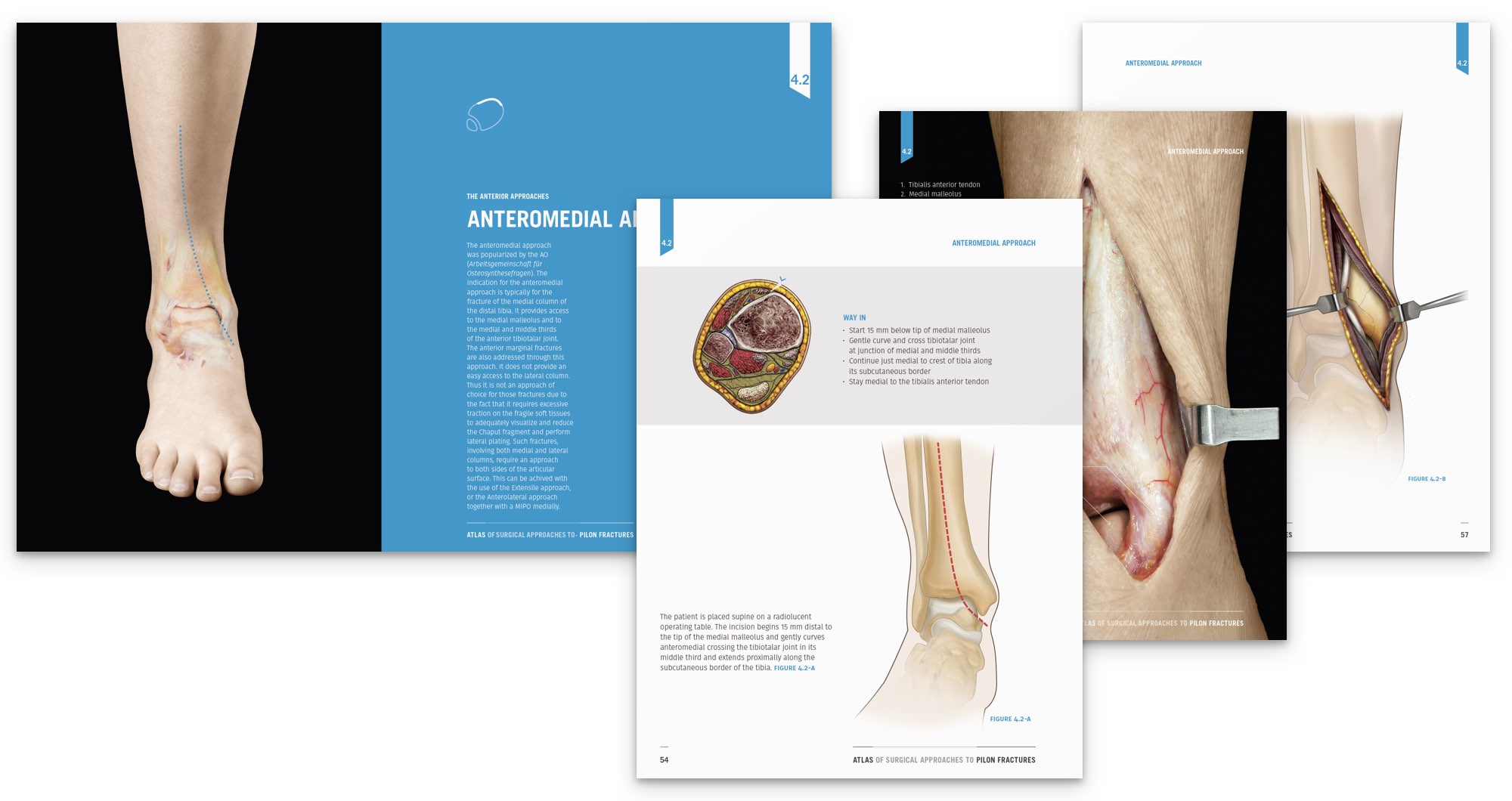
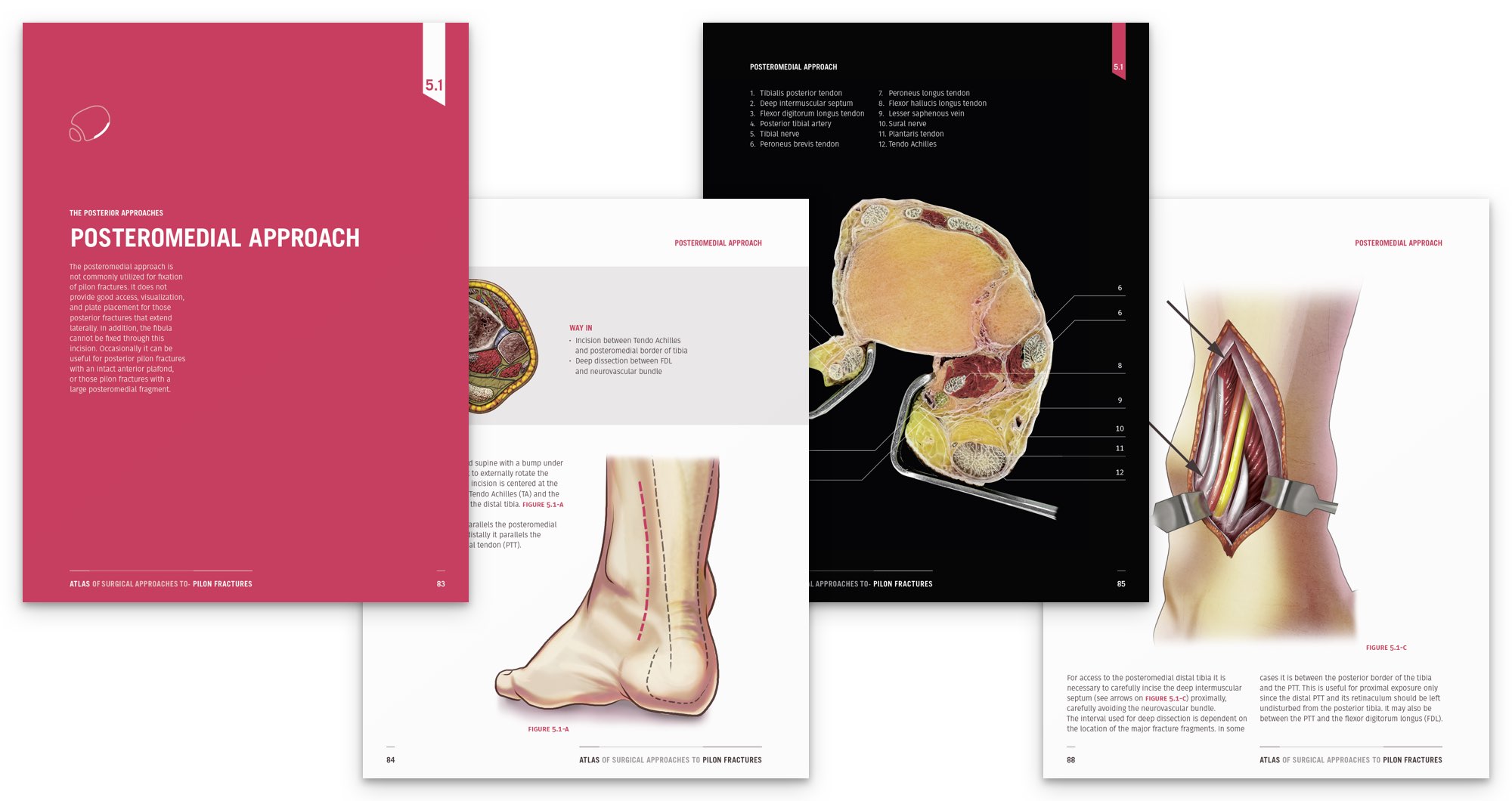
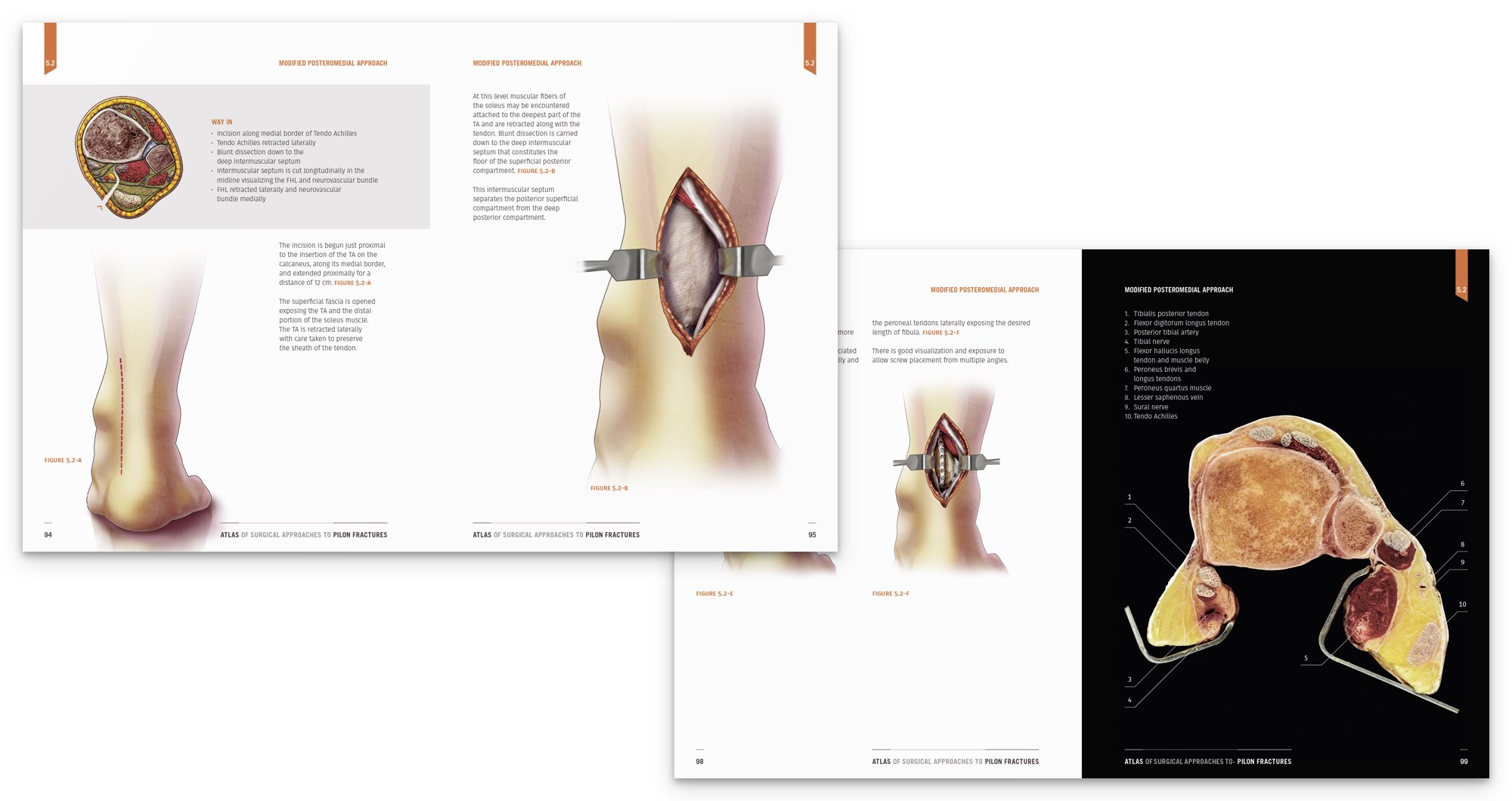
Table of Contents
Foreword by Pierre J. Hoffmeyer
Foreword by Hans Zwipp
Preface by Jean H.D Fasel
1. Introduction
2. Surgical anatomy
3. The Seven Surgical Approaches
4. Anterior Approaches

4.1. Minimally Invasive Approach
The minimally invasive approaches (Minimally Invasive Plate Osteosynthesis, MIPO) are indicated primarily for extraarticular fractures (AO/OTA 43-A, which are not pilon fractures), or distal tibia fractures with a simple split into the articular surface (AO/OTA 43-C1). They play very little role in fractures with any greater degree of articular involvement. The general objective with a less invasive approach is not to expose the metaphyseal component of the fracture so as to avoid disturbing soft tissue and bone vascularity.

4.2. Anteromedial Approach
The anteromedial approach was popularized by the AO (Arbeitsgemeinschaft für Osteosynthesefragen). The indication for the anteromedial approach is typically for the fracture of the medial column of the distal tibia. It provides access to the medial malleolus and to the medial and middle thirds of the anterior tibiotalar joint.
The anterior marginal fractures are also addressed through this approach. It does not provide an easy access to the lateral column.

4.3. Extensile Approach
The extensile approach is indicated for the group of fractures that result in a complete separation of the three columns of the tibia at the metaphysis or diaphysis. No portion of the articular surface remains in contact with the shaft and there is usually extensive joint comminution. Up until recently there was no single incision described that permitted simultaneous exposure of the medial and lateral columns.

4.4. Anterolateral Approach
The anterolateral approach is indicated for pilon fractures that involve the lateral column. It may be indicated in anterior and anterolateral AO Type B fractures, in AO Type C fractures with articular damage laterally, and in those cases with a valgus deformity thus requiring a lateral buttress plate. It provides the access to the lateral and middle thirds of the anterior tibiotalar joint, but does not provide access to the medial column.
5. Posterior Approaches
When to go Posterior?

5.1. Posteromedial Approach
The posteromedial approach is not commonly utilized for fixation of pilon fractures. It does not provide good access, visualization, and plate placement for those posterior fractures that extend laterally. In addition, the fibula cannot be fixed through this incision. Occasionally it can be useful for posterior pilon fractures with an intact anterior plafond, or those pilon fractures with a large posteromedial fragment.

5.2. Modified Posteromedial Approach
An option to expose the entire posterior pilon is to perform a modified posteromedial approach. This provides visualization from medial to lateral without extensive soft tissue retraction.
The cross-sectional anatomy of the pilon shows the surgical approach medial to the TA and FHL, and lateral to the neurovascular bundle.

5.3. Posterolateral Approach
The posterolateral approach has been well described. It is typically indicated for fracture of the posterior malleolus with a lateral fracture line, as well as for fractures extending into the incisura fibularis. It provides access to the lateral malleolus and to the lateral and middle thirds of the posterior tibiotalar joint.